Jan 21, 2026
Nov 25, 2025
A Genuine Commitment to Users Requires Rigorous Accountability
Matt Angle
The implantable brain-computer interface (BCI) industry is still in its early days. After 20 years of compelling academic clinical trials, there are now only a handful of mature companies working to bring implantable BCIs to market. The next decade will be a decisive test: these companies must simultaneously ensure the clinical and commercial success of their first products while developing the next generation of hardware that will expand the frontiers of the field.
In our recent blog “Think Fast,” we outlined the importance of robust preclinical benchmarks to speed device development and allow for objective comparisons across BCI platforms. Such tests are essential for rapid engineering progress. But engineering tests are not the whole story. The final validation of any BCI will come from the people who use it. The first opportunity for that feedback, both for companies and for regulators, will come through clinical trials.
That makes Clinical Outcome Assessments (COAs) central to the maturation of our field. The U.S. Food and Drug Administration defines COAs as measures intended to describe or reflect how a patient feels, functions, or survives. Here we describe two recent papers that represent the current state of regulatory science, and provide our own perspective from the standpoint of implantable BCI.
Redefining Independence in a Digital World
Mois and Rogers (2024) point out that the use of digital devices has become essential to daily modern living. As the world becomes increasingly digital, it affords a unique opportunity for technology to facilitate everyday activities—remote banking, digital health management, and social connectedness—but it also exposes a growing gap: traditional clinical outcome assessments no longer capture the full range of tasks and skills required for independent living.
To better reflect the realities of modern life, they introduce Digital Activities of Daily Living (DADLs), a framework recognizing that digital competence has become central to autonomy. DADLs build upon Activities of Daily Living (ADLs), which includes basic self-care tasks such as bathing, dressing, and eating, and Instrumental ADLs (IADLs), which encompass the more complex skills required for independent living, such as managing finances, preparing meals, or using transportation. DADLs include the digital tasks that are prerequisite to both, such as logging into a patient portal, paying bills online, or configuring a telehealth app.
The authors argue that digital ability is no longer optional but a determinant of well-being, safety, and social inclusion. They explain that DADLs disproportionately affect high-risk populations, particularly older adults with cognitive, physical or socioeconomic barriers, which places them at increased risk for reduced autonomy and diminished quality of life. By articulating DADLs as an additional domain of daily function, they recast digital literacy as a health variable and call for structured assessment tools, “digital caregivers,” and policy frameworks to bridge emerging disparities in digital access.
For many readers, this clinical hairsplitting may seem esoteric, but it directly informs how clinical trials are structured and what is considered “restoration of function” in the case of BCI. It will inform what regulators need to see to justify approval and what payers need to see to justify reimbursement. In short, the approach to measure a clinically relevant BCI outcome could greatly accelerate (or delay) market adoption of BCIs.
Measuring Digital Independence
More recently, Sawyer et al. (2025) take on the concept of digital activities from a more pragmatic lens. More than providing a theoretical framework, their paper seeks to operationalize digital function within the existing regulatory language of Instrumental Activities of Daily Living—introducing the Digital IADL Scale as a formal Clinical Outcome Assessment (COA).
Sawyer and colleagues argue that digital technology has changed how we carry out traditional ADLs and IADLs, making many existing clinical assessments feel outdated. While Mois & Rogers (2024) focus on older adults’ challenges with DADLs, Sawyer et al. broaden the conversation to people with significant physical disabilities, for whom digital interfaces are often the only way to manage tasks like shopping, banking, communication, and healthcare. Their key point is that if daily life has become digital, our tools for assessing daily function need to reflect that reality. It is not a philosophical exercise but a regulatory one – addressing how to measure functional independence for individuals whose interaction with the world is mediated through assistive or implantable technologies.
Using a multi-stage methodology that combines expert opinion with patient-centered input, the authors construct a graded scale capable of detecting partial independence and meaningful change—features essential for regulatory acceptance by the FDA and, eventually, by payers. For insurers and policymakers, this distinction is critical: embedding digital performance within an established functional hierarchy creates a pathway towards end points that can be eventually interpreted. Although the Digital IADL Scale described in this paper is still in early development and requires additional testing and validation, it illustrates the kind of purpose-built measure needed for BCI use cases. A scale tailored towards the functional realities of BCI users would allow the field to demonstrate not just technical performance, but meaningful, real-world capability—the kind of evidence that links technology access to reimbursement, value, and ultimately, adoption.
Importantly, the authors describe IADLs as more than checklists, they are graded scores from (1-6) representing the extent to which activities can be performed independently.
This paper is an important step in aligning BCI regulation and reimbursement with traditional clinical outcomes, which should translate into faster approval and reimbursement for devices.
Independence Alone is Not Enough—The Case for Measuring Performance
Sawyer et al. are not dogmatic about how IADLs should ultimately be scored, though they strongly suggest adopting the CARE scale used by CMS to assess degrees of independence. We believe this is an excellent starting point for evaluating functional restoration—but it is also incomplete. To fully capture the value of BCIs, outcome measures must reflect not only how independently an activity is performed, but also how well it is performed: the time required, the frustration or cognitive load involved, and the accuracy or errors observed. For example, a person could be “independent” in sending an email with a BCI, but if it takes them 30 minutes and is mentally exhausting, that’s very different from a system that allows them to do it in 2 minutes with ease. The CARE scale, as proposed, might not capture that crucial difference and thus, independence alone cannot capture these dimensions.
In practice, both regulators and payers will need measures that consider both independence and performance quality—metrics that can express not only whether a task is done, but whether it feels natural, efficient, and human. That distinction is subtle but vital, and it will shape how “restoration of function” is defined for the next generation of brain-computer interfaces.
To illustrate the importance of capturing both, consider four archetypal BCI systems:
- Low-independence, low-performance: These systems permit rudimentary interaction but not sustained autonomy—typified by early EEG-based interfaces that provided only coarse, slow control.
- High-independence, low-performance: These systems allow users to act independently, but only through narrow, low-bandwidth channels, e.g. composing a sentence after minutes of selection and confirmation. The interaction is technically autonomous but practically exhausting.
- Low-independence, high-performance: Here, richer output is possible, like continuous, high-resolution control of a cursor or text interface, but only under close supervision or in controlled clinical environments, where caregiver assistance remains essential.
- High-independence, high-performance: The ideal intersection of autonomy and fluency, where users can communicate and act naturally, with both speed and precision, in real-world contexts.
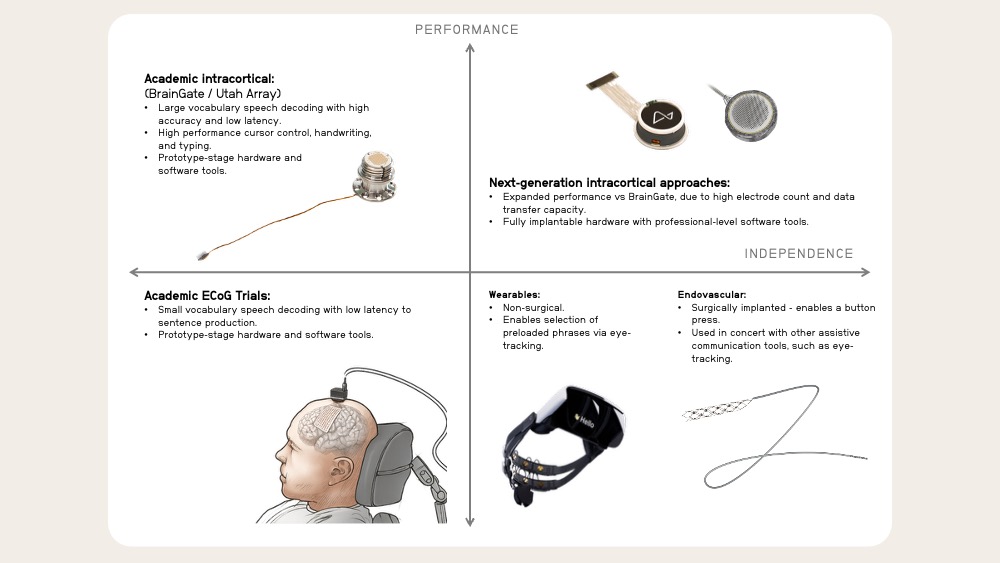
For those active in the field, it will be obvious that one prominent example of a high-independence, low-performance device already exists in clinical trials today, while most of the past twenty years of academic work have explored low-independence systems of variable performance.
At Paradromics, we believe any system of Clinical Outcome Assessment for BCI should incentivize progress toward high independence and high performance—which means graded scales for both must exist.
Restoring Connection
A recent paper by Van Balen et al. holds BCI to an even higher standard. Their concept of Relational Personhood reframes clinical success not simply as the restoration of capability, but as the restoration of connection. They argue that a person’s ability to express themselves allows others to perceive them as a full individual—and enables them, in turn, to perceive others the same way.
While the authors approach relational personhood through ethical and clinical lenses, we also read it as an engineering challenge. Providing capabilities and experiences that restore or recover feeling as well as function requires richer data (see our blog “The Speed of Thought”). Agency and embodiment emerge when the richness of the data matches the richness of real-world expression. When information flows freely and instantly, intentions are expressed in real time and interaction feels authentic. When the data link is narrow or delayed, rhythm and reciprocity break down.
To make this concrete—and to link the concept directly to measurable performance—consider that several BCI companies have identified communication restoration for people with severe paralysis as their first clinical application. Communication, at its core, is an information problem, and devices with different data rates enable fundamentally different kinds of communication capabilities:
- <2 bits per second → equivalent to access to one or two buttons that can be pressed once or twice per second.
- ~10 bits per second → enables smooth cursor control or text entry at keyboard speeds.
- ~40 bits per second → likely required for real-time, natural speech (not yet demonstrated clinically).
These numbers carry enormous human significance. Imagine a father with paralysis listening as his teenage daughter tells him she’s being bullied at school:
- With a low–data–rate BCI (1–2 bits per second), he types letter by letter. Each sentence takes minutes. The emotional rhythm dissolves into long silences, and what should be a moment of comfort becomes a test of endurance.
- With the same low-bandwidth system paired with AI assistance, he selects from prewritten replies. The words are fluent, even kind—but both know they were chosen by the machine.
- With a high-bandwidth speech prosthesis, he responds in real time—interrupting gently, reassuring naturally, even laughing softly at just the right moment. In that exchange, connection is restored.
Intracortical BCIs in clinical research studies are approaching this last threshold. We believe it is achievable in the near term with high-bandwidth, low-latency interfaces that carry enough information for conversational speech. In that sense, engineering fidelity is not only a technical goal but a moral imperative. As bandwidth and responsiveness improve, embodiment deepens—along with the ability to project intention, emotion, and presence.
Asserting Values, Engineering Success
As brain–computer interfaces move from laboratory experiments to commercial products, forums such as the iBCI-CC have seen healthy and sometimes spirited discussions about design philosophy in neurotechnology. Many of the major advances in this field originated in academic research, while most of the companies now working to translate them are backed by venture capital from the technology sector. This mix of cultures—clinical, academic, and entrepreneurial—has fueled extraordinary progress, but it has also raised a recurring concern: that the path from lab to market could drift away from the needs and lived experiences of patients.
Many implantable, clinical-stage devices are clearly higher performance than any non-implantable alternatives. The BrainGate program and recent Neuralink clinical trials have clearly demonstrated performance across a number of applications that would not be achievable in the same user population using non-implantable devices. For other devices, the advantages over non-surgical alternatives are less clear from a performance perspective. When questions about capability or data rate arise, the discussion too often shifts from evidence to narrative. In the most extreme positions that have been voiced, even the use of quantitative performance metrics has been dismissed as un-clinical or impersonal. In fact, the opposite is true; a genuine commitment to user needs requires rigorous accountability.
There is a false dichotomy between engineering-centric and patient-centric design in BCI. A company cannot be truly patient-centric unless it is engineering for performance. Rigorous measurement—of data rate, accuracy, stability, and subjective experience—is not at odds with empathy; it is its foundation. Without disciplined benchmarking, “patient focus” risks becoming a marketing slogan rather than a design principle.
Likewise, companies that claim their outcomes “can’t be quantified” are setting themselves up for short-term validation but long-term stagnation. For example, in the field of assistive communication, there have been suggestions from prominent figures that communication cannot be quantified in terms of bits. This is false. Indeed, the entire field of information theory developed from the telecommunications industry. Communication is an information problem; the degree to which a person can express themselves and feel present in interaction is bounded by the fidelity of that information channel.
When we bring the neurophysiology aspects of BCI into the conversation, we can also consider how intuitive that information channel is to control—e.g., is the BCI user thinking about kicking their leg to generate a button switch every second or are they thinking about speaking to generate speech?
Moving the field forward will require Clinical Outcome Assessments that reflect both data (technical performance) and a user’s lived experience of interaction—graded, continuous measures that enable quantitative comparison across devices while capturing how performance translates into human connection. The goal is not to reduce experience to numbers, but to ensure that those numbers point us toward technology that feels natural, responsive, and fully human.
Read more by Matt Angle on Substack.