Jul 23, 2026
Jun 2, 2026
When Going Deeper Pays Off
Electrical recording from the brain opens up a world of possibilities: from restoring speech to people who have lost it, to controlling neuroprosthetic limbs, to monitoring for conditions like epilepsy.
Implantable brain-computer interfaces (BCIs) are devices that are surgically placed inside of the skull, record brain activity, and process it to make it useful. But how exactly is the functionality of a BCI determined?
A deeper examination of BCI literature reveals that positioning in the brain is a key determinant of BCI functionality, demonstrated most evidently between the two prominent BCI modalities: intracortical and electrocorticography (ECoG).
Intracortical BCIs are implanted into brain tissue and directly interface with neurons, whereas ECoG sits at the surface of the brain and records neural data at a distance.
This difference in implant location determines everything, ultimately impacting a BCI’s applications and capabilities.
Neural Signal Architecture in the Motor Cortex
To understand why ECoG and intracortical modalities differ, we need to understand what brain data looks like. The fundamental unit of data measurement in the brain is called an action potential (AP), the “spark” across a neuron’s membrane that allows neurons to communicate with each other.
Research has shown that single neurons can have extremely precise tuning – for instance, one study of single-unit neuronal recordings revealed a neuron in an epilepsy patient that fired almost exclusively in response to images of Jennifer Aniston (Quiroga et al. 2005).
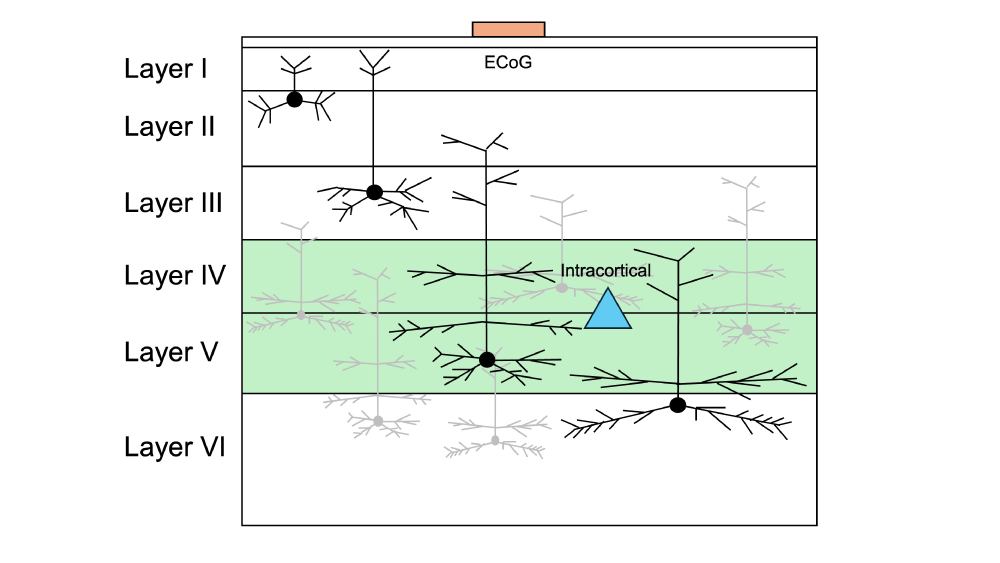
Illustration of different layers of the cortex in the brain. While some small pyramidal cells populate surface layers, dense populations of large motor neurons reside in layers 4-5 (highlighted in green). Positions of ECoG (orange rectangle) and intracortical (blue triangle) recordings are shown.
For the M1 motor region of the brain – a key target for high-functioning motor BCIs – this also holds true, given that individual corticospinal neurons can directly drive motor output (Cheney and Fetz 1980).
In the motor region specifically, the most salient information about movement is contained about ~1 mm below the surface of the brain (layers 4 and 5) (Wagstyl et. al, 2020; Parikh et al., 2009).
Thus, while individual action potentials from neurons can contain specific, unique information, in the case of motor neurons, that information might literally be buried quite deep.
Recording Modality and Signal Resolution
With the architecture of the brain in mind, let us now uncover what intracortical and ECoG devices record individually.
Intracortical devices directly record action potentials from individual neurons. Studies have shown that an electrode must be within ~30-100 μm of the target neuron to measure action potentials, or else signals become too weak and noisy (Gold et al. 2006; Letner et al. 2023).
Thus, by the nature of their implantation, intracortical devices are close enough to the neurons to record this rich information.
In contrast, ECoG is inherently unable to access single action potentials and instead must rely on an averaged signal from many different neurons; for instance, an ECoG electrode with a 1mm² contact averages on the order of over 50,000 neurons (Young et al. 2013).
Thus, ECOG does not measure information-rich action potentials, but rather an approximation of this data over a larger surface area.
Physical Constraints of Surface-Level Recording
Some proponents of ECoG-based BCI platforms make the claim that it doesn’t matter that you only record “averaged” neural activity because you can feed it into AI and enhance it back into the level of an action potential.
However, this solution fails to take into account the information limitations of ECoG data and the physics of neural recording.
The Brain’s the Limit
Not every signal transformation is experimentally reversible. For example, frosted privacy glass scatters light too much for curious passersby to peep into a first-floor apartment, even if they used special AI glasses.
To drive home this point with a closer physics analogy, let’s imagine you want to listen to a group of people living 40 miles below the surface of the earth in a doomsday bunker (similar to the motor neurons buried deep in the brain).
If you placed a very sensitive microphone to the ground, you could possibly hear a faint collective babble from the underground residents.
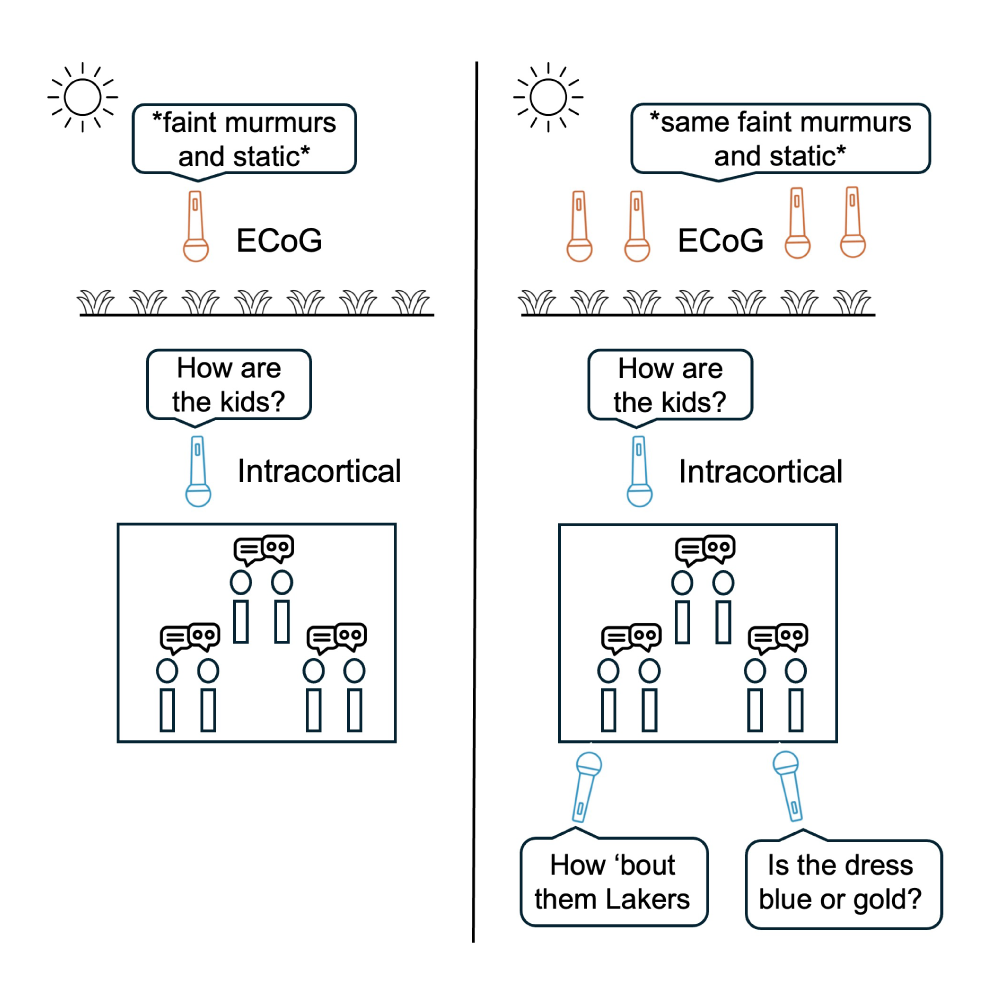
Underground bunker analogy. Increasing the number of ECoG electrodes at the surface records more averaged, noisy information; increasing the number of intracortical electrodes records new, distinct, high-quality information.
Since this recording is a mash up of voices, you could hear if the population is louder as a whole from this data (maybe they’re excited?), but you couldn’t get individual conversations from this data.
And adding more microphones won’t help; the data is so well mixed by the time it gets to the surface that the microphones record the same (or close to the same) signal.
Fine-tuned signals are lost through spatial averaging, and you simply can’t un-average data to get back the specific, rich action potentials from a single neuron in the same way you can’t un-bake a cake to figure out its ingredients (Buzsaki et al., 2012).
Physical Limitations in the Brain
This same reasoning applies for surface-level recordings of deep motor neurons. Physics-based models have found that the greater the distance from the neural signal, the weaker it is (this is also intuitive, of course) (Buzsaki et al., 2012; Einevoll et al., 2013).
Quantitative simulations suggest that at the cortical surface, action potentials from even superficial layers are attenuated to below detection thresholds (Hill et al., 2018).
With this in mind, let us compare an intracortical device within 100 uM of a neuron in Layers 4-5 versus an ECoG device at the surface of the brain, about ten times as far away from the neuron; signals sensed by the ECoG device would be at least 10 times weaker than the intracortical device.
In this sense, recording from an ECoG device would be like trying to hear someone talking to you from forty feet below the earth. It would be similar to asking: is someone shouting at me from an underground doomsday bunker? Or is it just the wind?
When More is not More
If ECoG records weaker, lower-quality signals, why not simply use more ECoG electrodes to get the same resolution as intracortical BCIs?
The answer is that even if you add more and more ECoG electrodes closely together they are still 1) far away at the surface of the brain and 2) largely just recording overlapping neural populations.
In fact, papers have modelled the amount of information gained from adding ECoG arrays (Trumpis et al. 2018), and two main scenarios have presented themselves in which more ECoG would equal more pertinent information (Hermiz et al., 2018):
- If the two devices were picking up the same signal, but different background noise
- If the two devices were picking up the same background noise but only one picked up the signal well
Both scenarios would allow you to refine your data to have stronger signal and less noise. But in reality, these two scenarios would not always be present, and it is highly likely that adding more ECoG devices would just result in more redundant information.
Even in the case of micro-ECoG, which uses electrode contacts under 250 microns at sub-millimeter spacing, you would just have more population-level data, not individual neuron data.
This contrasts with intracortical data; the performance of intracortical BCI decoders has been found to increase in a log-linear relationship with the amount of neuronal signals recorded at the same time (Schwartz et al. 2014); and a study found that doubling the amount of intracortical electrodes cuts performance error of a brain-to-speech BCI in half (Willett et al., 2023).
This log-linear relationship between electrodes and information applies specifically to intracortical BCIs because of their intrinsic design: since each electrode records individual neurons, and inter-neuron correlations are low (Smith and Fetz 2009), new electrodes add uncorrelated data sources and reduce decoding error.
Adding a ton of microphones/electrodes on the surface doesn’t change much, but going deeper adds uncorrelated data sources, which is fundamentally better.
Comparative Clinical Evidence for Intracortical over ECoG
These two caveats – that intracortical records action potentials and that ECoG records the summed activity of thousands of neurons – play out when we look at BCI applications that require a large amount of rich, high-dimensional, high-fidelity neural data.
In the case of neuroprosthetics to restore speech, ECoG BCIs must employ very complex decoding models that leverage entire sentence-level context to compensate for the lack of single-neuron information, which in turn leads to high computational power, multi-second delays, and more limited the user vocabularies.
This is supported by a 2026 pre-print from Emory University; when comparing an intracortical brain-to-text communication system to an analogous high-density ECoG system, the intracortical system had a 100x larger vocabulary for users to choose from, a 200x smaller footprint, and a similar stability to ECoG of over 2 years (Tomaszweski et al., 2026).
Intracortical outperformance of ECoG has also been repeatedly shown in peer-reviewed literature. In 2021, two studies came out: one for an ECoG BCI system (Moses et al. 2021) and one for an intracortical BCI system (Willett et al., 2021).
While both systems performed similarly – enabling participants to type at approximately 15 words per minute – these two systems had entirely different parameters.
The intracortical system allowed the user to type any word in the English language with an error rate less than 1%, while the ECoG system only allowed selection from a 50-word menu and had an error rate over 25%.
A similar scenario occurred again in 2023: in two separate studies of an ECoG system (Metzger et al., 2023) and an intracortical system (Willett et al., 2023), participants that were unable to speak used a BCI to convert brain signals from the motor and premotor cortex to text.
Both studies’ participants were able to generate text at word rates about half the speed of a normal speaker, and both error rates were around 25%. However, the intracortical system generated text from a list of 125,000 (the approximate vocabulary of an adult), with negligible delay between speaking intent and text generation.
In contrast, the ECoG system only generated text from a list of 1,024 words (the approximate vocabulary of a three-year-old) and had substantial delay between speaking intent and text generation.
Thus, while a superficial look at the research might find ECoG and intracortical equivalent in functionality, a deeper examination shows that intracortical emerges as superior for complex BCI indications.
Appropriate Clinical Applications for Each Modality
Upon examining the literature, one might ask: why pursue ECoG as a BCI modality at all when intracortical has demonstrated superior recording quality for single neurons and expanded BCI functionality?
A truly nuanced discussion would include that some ECoG proponents view intracortical as more “invasive” than ECoG, as it requires implanting directly into the brain, whereas ECoG stays “safely” at the surface.
However, this view is not backed up by the literature, which has shown both safe implantation of intracortical arrays in humans for years as well as safe explanation (Rubin et al. 2023).
Additionally, this view does not take into account that ECoG devices, as implanted today, must cover a 200x larger area of the brain in order to achieve decoding results that are still inferior to intracortical devices.
This surface area requirement isn’t without consequence, especially from a surgical perspective. It either involves a larger craniotomy or “blind insertion” of the device under the skull without direct visualization, both of which are largely untested surgical methods.
To categorically characterize ECoG as “safer” than intracortical is simplistic at best, which we discuss more in our upcoming safety blog.
Beyond the “safety” argument, there is a legitimate argument to be made that ECoG, while underperforming in complex tasks, could be useful for other specialized tasks that require monitoring at a higher level for a large geographical area of the brain.
In fact, ECoG has decades of validated clinical use for identifying and monitoring areas for seizure onset and mapping their propagation across the brain (Alshahrani et al., 2025).
Additionally, ECoG could be used for functional cortical mapping pre-surgery, where stimulation through ECoG electrodes during prompted patient tasks allows for identification of language/motor areas for each individual patient.
Furthermore, ECoG could excel at monitoring high-level neuron populations associated with attention, cognitive state, and sleep dynamics.
Thus, while intracortical devices may surpass ECoG in BCI applications that require high-fidelity, rich information to manipulate neuroprosthetics with a high degree of freedom and agency, this is not the only use case for BCIs, and ECoG could indeed fill other niches well.
Stability of Intracortical versus ECoG Recordings
While it is true that historical intracortical recording platforms have had longevity issues, this does not extrapolate to all intracortical devices.
Device longevity can be impacted by neural immune response, where glial cells form encapsulations around implanted electrodes, gradually degrading signal strength and quality over time (Kozai et al. 2015).
Immune response is strongly modulated by the physical characteristics of the device. The glial cell / astrocytic response is particularly sensitive to electrode diameter (Thelin et al. 2011).
Early generation Utah arrays have electrode diameters of 100 uM, which have been found to lose signal over time due to biological disruption and accelerated electrode degradation (Sponheim et al. 2021).
In contrast, Paradromic’s next-generation electrodes are 40 uM in diameter and have achieved stable intracortical recordings for years, as measured both by single-channel SNR and total system information transfer.
This is not to say that newer versions of intracortical electrodes have no impact on tissue or neural circuits, but these advances in electrode design have optimized their safety and longevity.
Similarly, in the early days of intracortical recording, decoders were sensitive to day-to-day changes in single neuron signals, which caused loss of function over time and required frequent recalibration.
Modern decoders (Degenhart 2020, NoMAD) are much more robust against electrode drift issues, and with proper implementation, they do not require supervised recalibration at all.
A Depth of Knowledge in Intracortical Devices
When we go beyond the surface level and take a deep dive into neurophysiology, academic research, and clinical studies, intracortical BCIs clearly emerge as the superior modality when compared one-to-one to ECoG for high-degree-of-freedom functionality.
This is exactly what guided the design of our intracortical Connexus® BCI device, which, accordingly, has the highest measured data rates for a BCI system.
Thus, it goes to show that it will take going deeper, both physically and metaphorically, to push BCI applications to the next level.